In my practice, I regularly treat patients whose bodies respond to manual lymphatic drainage with flushing, hives, or unexplained swelling flares. These are not typical reactions. When a patient's skin turns red during a session, or hives appear along the treatment area, it tells me something important: their lymphedema may not be the only condition we are managing. Their mast cells may be involved.
I see this pattern often enough that it shapes how I approach certain patients from the very first visit. Many of these individuals have an underlying condition called mast cell activation syndrome (MCAS), whether they know it or not. Some also live with hypermobile Ehlers-Danlos syndrome (hEDS), and the overlap between these conditions and lymphedema is more common than most clinicians realize.
If you have ever experienced unexplained flushing, hives, or swelling flares during or after lymphatic drainage, or if you live with hEDS alongside your lymphedema, this post is for you. Understanding the connection between mast cell activation and lymphatic dysfunction is changing how I approach treatment for some of my most complex patients at my clinics in Leesburg and Ashburn, Virginia. It should be changing how your care team thinks about your swelling, too.

What Are Mast Cells and Why Should You Care About Them?
Mast cells are immune cells that live in your connective tissue, particularly in your skin, your gut lining, and around your blood and lymph vessels(1). Think of them as your body's first responders. When they detect something they perceive as a threat (an allergen, an infection, a physical trigger like heat or pressure), they release a burst of chemical mediators from tiny granules stored inside them. This process is called degranulation.
The most familiar of these mediators is histamine, the molecule behind itching, flushing, hives, and the swelling you associate with an allergic reaction. But mast cells release far more than just histamine. They also release tryptase (a protein that can stimulate fibroblasts to produce collagen), prostaglandins, leukotrienes, and cytokines like TNF-alpha and TGF-beta(2). These molecules drive inflammation, attract other immune cells, dilate blood vessels, and, critically for my lymphedema patients, promote tissue fibrosis.
In a healthy immune system, mast cells activate when they are supposed to and calm down when the threat passes. In mast cell activation syndrome (MCAS), that "off switch" is broken. The cells fire too easily, too often, and in response to triggers that should not provoke a reaction at all(3).
Why this matters for lymphedema: mast cells are concentrated around lymphatic vessels. When they degranulate, the histamine, tryptase, and TGF-beta they release can increase vascular permeability (causing more fluid to leak into tissue), drive fibrosis in lymphatic collecting vessels, and impair the lymphatic system's ability to clear fluid(4). In other words, overactive mast cells do not just cause allergic symptoms. They can actively worsen your lymphedema.
What Is MCAS, and What Is the "Trifecta" I Keep Hearing About?
Mast cell activation syndrome is a condition in which mast cells release their mediators excessively or inappropriately, producing a wide range of symptoms across multiple body systems(3). These can include flushing, hives, unexplained swelling, abdominal cramping, brain fog, rapid heart rate, low blood pressure, and reactions to foods, temperatures, or physical pressure that seem to come out of nowhere. Many patients describe it as feeling like their body is allergic to itself.
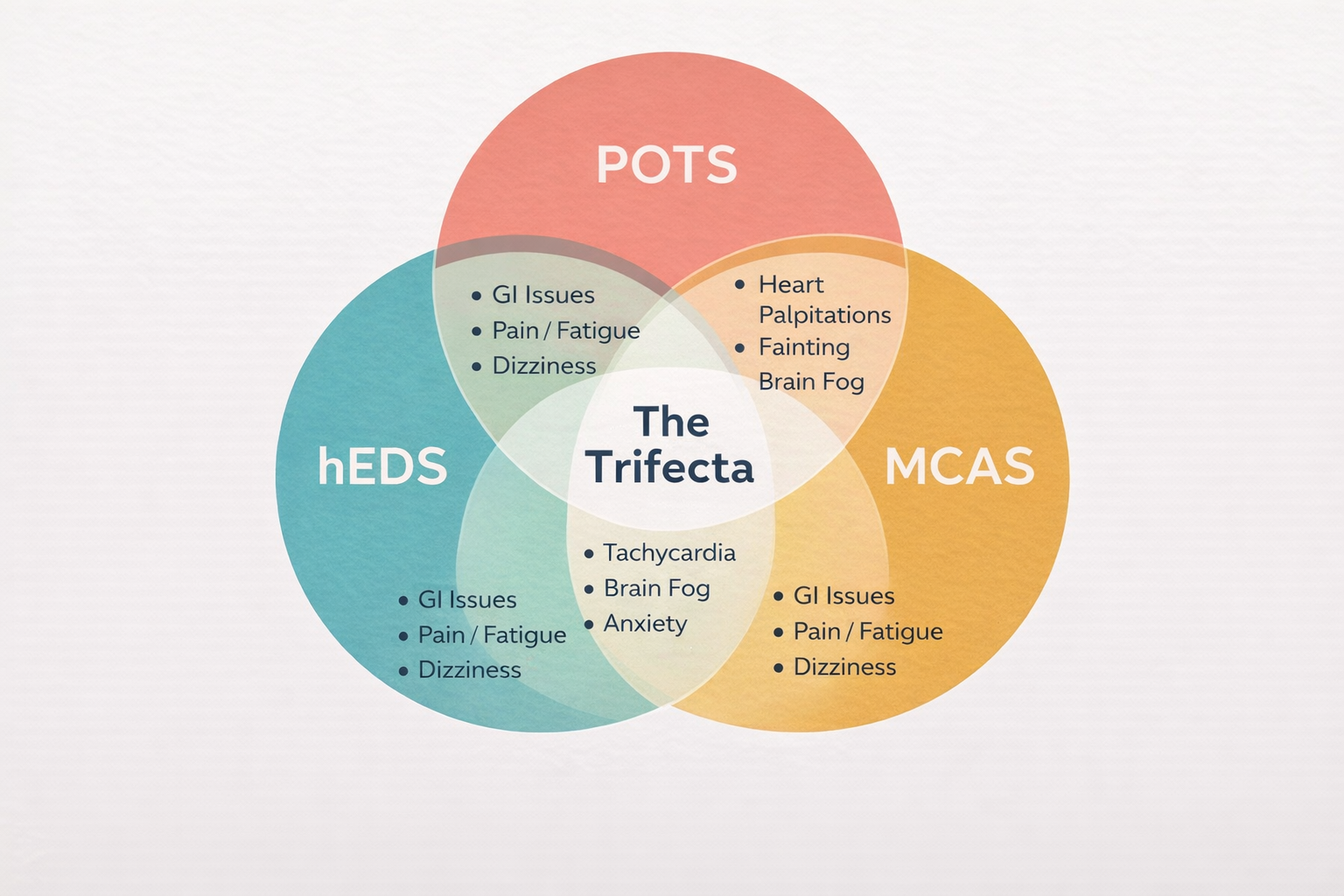
MCAS is increasingly recognized as part of what clinicians and patients call "the trifecta": the co-occurrence of hypermobile Ehlers-Danlos syndrome (hEDS), postural orthostatic tachycardia syndrome (POTS), and mast cell activation syndrome(5). In my practice, I see this overlap regularly. A patient comes in for lymphedema management, and during assessment I notice fragile, hyperextensible skin, joint hypermobility, a history of easy bruising, and unexplained reactions to touch or temperature. These are not coincidences. They are clues.
The connective tissue fragility in hEDS affects the structural integrity of lymphatic vessels themselves. When you combine that with the chronic inflammation driven by overactive mast cells and the circulatory instability of POTS, you have a patient whose lymphatic system is under assault from multiple directions at once. The relationship between mast cell activation syndrome and lymphedema is not a coincidence in these patients. It is a mechanistic connection. Managing the lymphedema without accounting for the mast cell component is like mopping a floor while the faucet is still running.
How Do Mast Cells Make Lymphedema Worse?
This is where the science gets specific, and where I want to give you the real picture, not a simplified version that leaves out the mechanisms your body is actually dealing with.
Research has shown that lymphedematous tissue contains significantly more mast cells than healthy tissue(4). These mast cells are not passive bystanders. They are actively releasing tryptase, a protease enzyme that stimulates fibroblast proliferation and collagen synthesis(6). That means more mast cell activity equals more fibrosis, more tissue hardening, and more resistance to treatment.
The fibrosis pathway works through a signaling molecule called TGF-beta (transforming growth factor-beta). TGF-beta is one of the body's primary drivers of scar tissue formation and extracellular matrix buildup(7). In lymphedema, elevated TGF-beta increases fibroblast stiffness, impairs the formation of new collateral lymphatic vessels, and promotes the deposition of type I and type III collagen in the affected tissue(8). The result is the dense, non-pitting tissue that characterizes Stage 2 and Stage 3 lymphedema.
Here is the critical connection: mast cells are a significant source of TGF-beta in lymphedematous tissue(6). When mast cells degranulate, they release both tryptase and TGF-beta, which together drive a fibrotic cascade. Tryptase stimulates fibroblasts directly. TGF-beta amplifies the process by promoting fibroblast-to-myofibroblast transition, essentially turning your tissue's repair cells into scar-producing cells. This is not speculative. It has been demonstrated in biopsy studies of secondary lymphedema patients(6).
For patients with MCAS, where mast cells are degranulating more frequently and more aggressively than normal, this fibrotic pathway is effectively on overdrive. That is often why some patients progress to fibrotic lymphedema faster than their clinical picture would predict, and why standard Complete Decongestive Therapy alone may not be enough.
The clinical implication is clear: if you are treating lymphedema without considering mast cell involvement, you may be addressing the fluid but missing the fibrosis. Both need attention.
What About Post-Surgical and Cancer-Related Lymphedema?
For my patients with cancer-related lymphedema, the mast cell picture adds another layer. Radiation therapy and the tumor microenvironment itself significantly increase mast cell density in the affected tissue(9). I see the downstream effects of this regularly: accelerated fibrotic changes in the irradiated limb, complicated wound healing in patients with skin breakdown, and inflammatory flares that can look and feel remarkably like cellulitis but are actually mast cell-mediated responses.
Distinguishing between a true cellulitis infection and a mast cell-driven inflammatory flare is one of the more nuanced clinical decisions in lymphedema care. Both present with redness, warmth, and swelling. But mast cell flares tend to come on faster, resolve without antibiotics, and are often triggered by identifiable factors like heat exposure, stress, or certain foods. Getting this distinction right matters, because the treatment paths are very different.
How Does Vodder Method Lymphatic Drainage Help (and When Should It Be Modified)?
One of the most common questions I hear from patients researching this topic is: is lymphatic massage safe with MCAS? The answer depends entirely on what kind of lymphatic work you are receiving, and from whom.
Here is where my training in the Vodder method becomes especially relevant. There is emerging evidence that manual lymphatic drainage may actually modulate mast cell activity(10). The gentle, rhythmic skin stretching that defines the Vodder technique (operating at pressures below 60 mmHg) stimulates mechanoreceptors in the skin. These mechanoreceptors can have a calming effect on local mast cell degranulation, which may partly explain why patients report reduced pain and inflammation after MLD beyond what simple fluid movement would account for.
This is an area of active research, and I want to be honest about what we know and what we are still learning. The anti-inflammatory and analgesic effects of Vodder MLD have been documented clinically for decades, but the precise mast cell mechanisms are still being mapped. What I can tell you from my own practice is that the gentle approach matters enormously for these patients. Vodder MLD is not deep tissue massage. It is not aggressive. It is precisely calibrated to work with your lymphatic system, not overpower it.
That said, for patients with known or suspected MCAS, I modify my approach. Many patients ask me: why does lymphatic drainage cause flushing? In most cases, the flushing reflects local vasodilation from histamine release as mast cells respond to the mechanical stimulus of touch. In patients without MCAS, this is mild and transient. In patients with MCAS, it can escalate. That is why I may shorten session duration, reduce the treatment area, start with proximal (closer to the trunk) work before moving distally, and closely monitor for signs of mast cell activation throughout the session: flushing, hives, itching, rapid heart rate, or a sudden feeling of being unwell. If those signs appear, I adjust immediately. Too much, too fast is the enemy of progress in this population.

This is one of the most important distinctions in my practice: the difference between a spa-style "lymphatic massage" that uses deep, aggressive pressure and the clinical Vodder technique that operates at feather-light pressures below 60 mmHg. For patients with mast cell sensitivity, that distinction is not a preference. It is a safety consideration.
When Do I Suspect Mast Cell Involvement in My Lymphedema Patients?
Not every lymphedema patient has MCAS, and I am careful not to over-label. But there are clinical patterns that prompt me to consider whether lymphedema flare triggers involve mast cells, especially when a patient's response to treatment is not following the expected trajectory.
| What I See in the Clinic | What It May Mean |
|---|---|
| Patient develops flushing or hives during MLD | Possible MCAS; I adjust session intensity, duration, and monitor closely |
| hEDS patient presenting with lymphedema | The trifecta (hEDS, MCAS, POTS) is common; I treat conservatively and screen for the full picture |
| Fibrotic, non-pitting lymphedema progressing faster than expected | Chronic mast cell-driven TGF-beta fibrosis may be accelerating tissue changes |
| Post-radiation lymphedema with frequent inflammatory flares | High mast cell density in irradiated tissue; distinguish from cellulitis before treating |
| Unexplained edema exacerbations that do not correlate with activity or diet | Consider mast cell triggers: stress, certain foods, heat exposure, hormonal shifts |
When I suspect mast cell involvement, my role is not to diagnose MCAS. That is the domain of immunologists and allergists, and I am grateful for the ones I collaborate with in the Northern Virginia area. My role is to recognize the clinical signals, modify my treatment approach to keep the patient safe and comfortable, and connect them with the right specialists when referral is warranted. Understanding the mast cell pathophysiology behind these presentations positions me to do all three.
How I Approach Lymphatic Drainage for Patients with MCAS
When a patient with known or suspected MCAS comes to my lymphedema practice in Leesburg and Ashburn, the treatment plan looks different from a standard CDT protocol. Manual lymphatic drainage for mast cell activation patients requires a recalibrated approach, not because the fundamentals change, but because the pacing, intensity, and monitoring need to account for a nervous system and immune system that react more easily.
I use the Vodder method exclusively for these patients. The feather-light, rhythmic strokes of Vodder MLD are specifically designed to work within the superficial lymphatic plexus without triggering the deeper tissue responses that can provoke mast cell degranulation. I start with shorter sessions (sometimes 20 to 30 minutes instead of the standard 45 to 60) and build duration gradually based on the patient's tolerance.
I also pay close attention to environmental triggers. Room temperature, fragrance exposure, and even the pressure of compression garments can provoke a flare in sensitive patients. For patients with fragile hEDS skin, I modify bandaging materials and monitor for pressure injuries that would not occur in patients with typical connective tissue.
The goal is never to push through a reaction. The goal is to find the therapeutic window where lymphatic drainage is effective without crossing the threshold that activates a mast cell response. That window is different for every patient, and finding it requires clinical experience, close observation, and the willingness to go slow when slow is what the body is asking for.

Building the Right Care Team When MCAS and Lymphedema Overlap
I want to be direct about this: no single provider solves this alone. The intersection of mast cell activation and lymphatic dysfunction requires collaboration, and the patients who do best are the ones whose providers communicate with each other.
In my practice, I coordinate closely with immunologists and allergists when MCAS is suspected or confirmed. They manage the pharmacological side: H1 and H2 antihistamines, mast cell stabilizers like cromolyn sodium, and, when indicated, targeted therapies like omalizumab. I manage the lymphatic side: Vodder MLD, modified compression, decongestive exercise, and skin care protocols adapted for sensitive or fragile tissue.
For patients with the full trifecta (hEDS, POTS, MCAS), I may also coordinate with cardiologists managing the autonomic dysfunction, geneticists or rheumatologists overseeing the connective tissue disorder, and pain management specialists. Each provider addresses a different piece of the puzzle. My job is to make sure the lymphatic management piece does not inadvertently provoke a mast cell flare while still achieving meaningful volume reduction.
If you are a patient reading this and thinking "nobody has ever connected these dots for me before," you are not alone. MCAS is underdiagnosed, and its overlap with lymphedema is still a relatively new area of clinical focus. The fact that you are learning about it now means you can bring these questions to your care team. And if you are in the Leesburg, Ashburn, or Northern Virginia area, my clinic is built for exactly this kind of complexity.
The Bottom Line: Your Swelling Might Be Telling You More Than You Think
Lymphedema is not always just lymphedema. When swelling flares unpredictably, when tissue hardens faster than expected, when standard treatment helps but never quite enough, the mast cell connection is worth exploring. The cytokines involved (histamine, tryptase, TGF-beta, TNF-alpha) are not abstract laboratory concepts. They are molecules actively shaping how your tissue responds to treatment, and understanding them gives both you and your care team a more complete picture of what your body needs.
I am one of a small number of Certified Lymphedema Therapists in Northern Virginia who specifically provides Vodder lymphatic drainage for MCAS patients as part of an integrated treatment approach. This is not because the knowledge is secret. It is because the overlap between lymphatic medicine and immunology is only now receiving the clinical attention it deserves. The patients who benefit most are the ones whose providers are willing to look beyond the swelling and ask what is driving it.
If any of this resonates with your experience, visit my Certified Lymphedema Therapist page to learn more about how I approach complex lymphatic conditions, or call (703) 637-8252 to schedule a consultation.
In health,
Dr. Grace Villaver, DPT, CLT
Level Up Rehabilitation Services, LLC
42910 Winkel Dr, Unit #105, Ashburn, VA 20147
(703) 637-8252 | Mon-Fri, 7 AM - 5 PM
References
- (1) Mast Cell Activation Syndrome Update: A Dermatological Perspective. PMC. pmc.ncbi.nlm.nih.gov
- (2) Mast cell activation disease: a concise practical guide for diagnostic workup and therapeutic options. PMC. pmc.ncbi.nlm.nih.gov
- (3) Mast Cell Activation Syndrome (MCAS). American Academy of Allergy, Asthma & Immunology. aaaai.org
- (4) Pathological Changes of Lymphedematous Skin: Increased Mast Cells, Related Proteases, and Activated Transforming Growth Factor-beta 1. Lymphatic Research and Biology. liebertpub.com
- (5) The Pentad Super Syndrome (hEDS, MCAS, POTS overlap). The EDS Clinic. eds.clinic
- (6) Tryptase-Positive Mast Cells Promote Adipose Fibrosis in Secondary Lymphedema through PDGF. MDPI/PMC. pmc.ncbi.nlm.nih.gov
- (7) Transforming Growth Factor-beta Signaling in Fibrotic Diseases and Cancer-Associated Fibroblasts. PMC. pmc.ncbi.nlm.nih.gov
- (8) TGF-beta 1 mediates pathologic changes of secondary lymphedema by promoting fibrosis and inflammation. PMC. pmc.ncbi.nlm.nih.gov
- (9) Mast Cell Activation Syndrome and Its Impact on the Lymphatics. Lympha Press. lymphapress.com
- (10) Mast Cells' Role, Lymphatic System, and Mast Cell Activation Syndrome. Perea Clinic. pereaclinic.com
- (11) Mast cell activation syndrome: Current understanding and research needs. PMC/JACI (Castells et al., 2024). pmc.ncbi.nlm.nih.gov
- (12) Certified Lymphedema Therapist: Vodder Method MLD. Level Up Rehabilitation Services. levelupptdoc.com
